 Actively Managed Equity
Actively Managed Equity Overview: All Strategies
Overview: All Strategies Investor Resources
Investor Resources Indexed Equity
Indexed Equity Private Equity
Private Equity Digital Assets
Digital Assets Invest In The Future Today
Invest In The Future Today
 Take Advantage Of Market Inefficiencies
Take Advantage Of Market Inefficiencies
 Make The World A Better Place
Make The World A Better Place
 Articles
Articles Podcasts
Podcasts White Papers
White Papers Newsletters
Newsletters Videos
Videos Big Ideas 2024
Big Ideas 2024
For more than a century, surgery and poison have been the antidotes to cancer. When tumors are discovered, doctors decide whether or not to remove them surgically. With or without surgery, doctors typically prescribe chemotherapy in an attempt to eradicate the disease chemically. Immunotherapy is the most heralded cancer treatment of the last 20 years, offering significantly better odds of survival.
If we look at chemotherapies, we see an unimpressive track record. Efficacy studies have shown response rates of around 13% for kidney cancer and 15% for glioblastoma, a form of brain cancer. Targeted therapies are better. For B-Cell malignancies targeted treatments are in the range of 50-72%.
Immunotherapy activates the body’s immune cells to fight cancer. Recent approvals of first-of-a-kind drugs from Amgen [AMGN], Bristol-Myers Squibb [BMY], and Merck [MRK] have attracted market attention. Additionally, Kite Pharma [KITE] and Juno Therapeutics [JUNO] each have market capitalizations over $2 billion despite a lack of products past phase II trials. As shown below, competitors are at different stages of capturing segments of the immunotherapy market.[1]
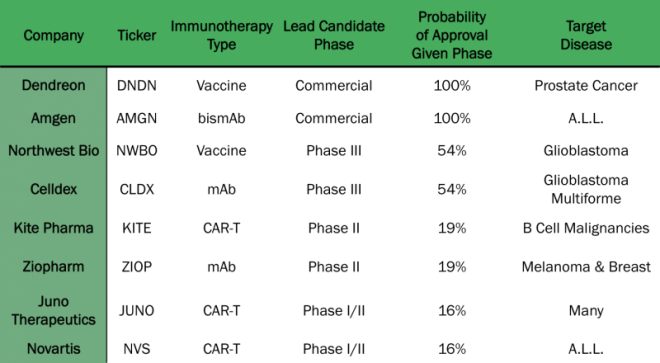
Bispecific monoclonal Antibody (mAb)
Monoclonal Antibody (mAb)]
Typically, tumors masquerade as normal tissues, fooling the immune system. Now, however, a number of leading candidate therapies expose and attack tumor cells for what they are, killers. Among them are CAR-T, cancer vaccines, cytokine therapy, and monoclonal antibodies, as shown below.
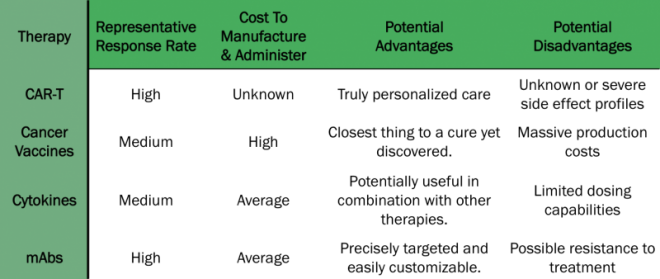
CAR-Ts, chimeric antigen receptor T-cells, modify immune cells to express receptors matching proteins on the surface of tumors. Patients’ t-cells are removed, edited to express the desired receptor, duplicated until there are billions of them, and re-injected into the patient. Novartis [NVS], Kite, and Juno have demonstrated complete remissions and response rates approaching 90% in leukemia. Despite successes, two patients died in an early Juno study, resulting in a temporary clinical hold. Further, the cost to produce the CAR-T treatments for large patient populations could be prohibitive.
Like CAR-T therapies, cancer vaccines attempt to harness immune cells to fight cancer. Vaccines focus on dendritic cells, the immune system’s most powerful antigen receptors. Because the therapy involves manipulating difficult cells after removing them from the patient, a vaccine can be both expensive and time consuming to produce. The only approved cancer vaccine is Dendreon’s (DNDN) Provenge, which has disappointed commercially due to high production costs. Northwest Biotherapeutics’s (NWBO) DCVAX-L is in Phase III trials, and its commercial fate remains to be seen.
CAR-T and vaccines both require novel drug production processes. Unlike other types of cancer drugs, the patient’s immune system is an integral part of the therapy. The ability to manufacture personalized drugs at scale could be a significant obstacle.
Cytokine therapy alters the immune cell pathways. Interleukin 2 (IL-2) is one example of cytokine therapy, and has been used commercially for cancer treatment dating back to Cetus Corporation in the 1980s. Cytokine therapy highlights cancer cells by elevating levels of IL-2, sending the immune system into overdrive. The problem with IL-2 and other cytokines is the narrow therapeutic window. Increasing dosage leads to significantly worse side effects. Thus, treatment cannot be escalated to improve outcomes.
Monoclonal antibodies (mAbs) bind to tumor cells to treat cancer precisely without harming healthy tissue. In development for years, multiple drugs are available commercially. These drugs bind to specific proteins on the surface of cancers cells, providing treatments in a number of ways. Some mAbs bind with immune cells to make the cancer more visible to the immune system. Others block cell growth signals. Still others deliver chemotherapy compounds to tumor sites.
Naked, conjugated, and bispecific are the primary subtypes of mAbs. Naked mAbs work on their own and, unlike conjugated mAbs, are not linked to other compounds such as chemotherapy or radioactive molecules. Bispecific mAbs (bismAbs), like Amgen’s Blincyto, contain two mAbs, binding multiple proteins to increase the efficacy of the treatment at lower doses.
The mAbs subtypes are important when assessing efficacy and the competitive landscape. For safety reasons, doctors prefer naked mAbs to radioactive conjugated mab, assuming equivalent efficacy. Likewise, CAR-T, vaccines, and mAbs are preferable to cytokines, as they accommodate higher doses.
At one time, knives and chemicals were the only weapons available to fight cancer. Now, however, the body’s immune system is being unleashed to fight cancer. Therapies with maximal efficacy and minimal side effect profiles will be the most promising medically and commercially. While still in nascent stages, personalized immunotherapy is on the leading edge of precision medicine, as cancer continues to evolve from a killer to a chronic disease.
Related Research


